Wiki Page
- Retina
- ROP
- RetCam
- ROP
- ROP Zones
- Immature Retina
- Stage 1 ROP
- Stage 2 ROP
- Stage 3 ROP
- Stage 4 ROP
- Stage 5 ROP
- ROP Plus Disease
- Type 1 ROP
- Type 2 ROP
- ARROP
- Pre-threshold ROP
- Threshold ROP
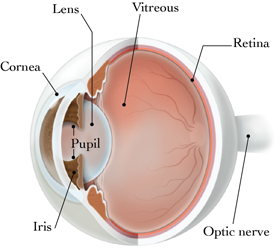
Retina
The retina is a nerve layer at the back of your eye that senses light and sends images to your brain. An eye is like a camera. The lens in the front of the eye focuses light onto the retina. You can think of the retina as the film that lines the back of a camera like wallpaper. The retina needs to be flattened against the back wall of the eye in order to function.
ROP
Retinopathy of Prematurity (ROP) is a blinding eye disease of premature babies and very low birth weight infants.
Retinopathy of Prematurity or ROP is a vasoproliferative disease affecting the retina of premature babies and very low birth weight infants. The eyes of premature babies can be screened and if detected early can be treated in time. Lack of ROP screening and timely laser treatment can lead to advanced ROP and poor prognosis. ROP is an important cause of blindness in developing countries.
RetCam
Retinopathy of prematurity (ROP) is a vision-threatening vaso-proliferative condition of premature infants worldwide. As survival rates of younger and smaller infants improve, more babies are at risk for the development of ROP and blindness. Meanwhile, fewer ophthalmologists are available for bedside indirect ophthalmoscopy screening examinations. Remote digital imaging is a promising method with which to identify those infants with treatment-requiring or referral-warranted ROP quickly and accurately, and may help circumvent issues regarding the limited availability of ROP screening providers. The Retcam imaging system is the most common system for fundus photography, with which high-quality photographs can be obtained by trained non-physician personnel and evaluated by a remote expert. It has been shown to have high reliability and accuracy in detecting referral-warranted ROP, particularly at later post-menstrual ages. Additionally, the method is generally well-received by parents and is highly cost-effective.
ROP Zones
International Classification of Retinopathy of Prematurity divided retinopathy of prematurity into 3 zones on the retina of the eye so as to facilitate clear communication between ROP experts. There are 3 Concentric Zones, wherein each zone is centered on the optic disc (head of the optic nerve) and normal retinal vessel development proceeds outward from the center of the optic disc toward the extreme periphery of the retina.
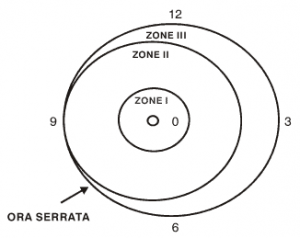
Zone 1 – Circle from centre of disc with radius of twice distance from disc to macula
Zone 2 – From nasal edge of zone 1 to ora nasally and upto equatot region of retina temporally
Zone 3 – From temporal crescent of retina anterior to zone II
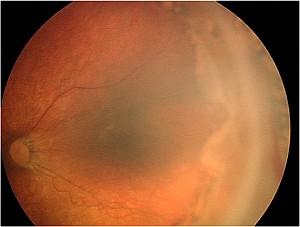
Immature Retina
Immnature retina is incomplete retinal vessel development, but not ROP. The eye goes through a normal vessel development with retinal vessels grow from the optic nerve head towards the retinal periphery. If they grow normally, they reach the nasal retinal peiphery (ora seratta) by 36 weeks post conceptional age and temporal periphery by 40 weeks post conceptional age.
This is a stage of no retinopathy of prematurity. These vessels can grow normally or later get stopped to develop ROP.
Stage 1 ROP
Stage 1 retinopathy of prematurity (ROP) signifies development of a demarcation line between the normal retinal vessel developed retina and avascualr retina, where vessels have not developed.
Stage 2 ROP
Stage 2 retinopathy of prematurity (ROP) signifies development of a demarcation ridge between the normal retinal vessel developed retina and avascualr retina, where vessels have not developed. The demarcation line of stage 1 gains height and width and extends above the retina surface.
Stage 3 ROP
Stage 3 retinopathy of prematurity (ROP) signifies development of a new vessels (neovascularization) in the stage 2 demarcation line and leads to extraretinal proliferation of tissue. The ridge may now bleed and cause traction on the ridge.
Stage three is a critical stage in development of ROP as it signifies that retinal ischaemia is significant enough to cause development of new vessels in an attempt to supply oxygen to this retina. However since retinal vessels are not there in the avascular retina in the periphery, the new vessels grow in a futile attempt to try to re-vascularise the area.
Extensive development of new vessels causes them to grow into the vitreous gel in the middle of the eye, which incites fibrous proliferation which eventually causes traction over the Ridge and can lead to retinal detachment. Extensive stage three ROP progresses through stages of prethreshold ROP to threshold ROP.
Development of stage three is critical for analysis of type I ROP, which is the current guidelines for treatment. Laser treatment can effectively reduce the development and progression of new vessels in the retina and can lead to regression of the disease.
It is very important for retinal specialists to identify and treat the disease as early as possible to prevent further complications.
Stage 4 ROP
Stage 4 retinopathy of prematurity (ROP) signifies that retinal detachment has started to occur due to the traction of the fibrous and vascular tissue over the ridge. Its called 4A when the retinal detachment spares the macula, and stage 4B when retinal detachment involves the macula.
Macula is the central part of the retina which contains the fovea which is essential for a clear vision in the eye. Any distortion of the macula or any macular detachment will lead to a decrease in vision. Therefore it is very important to control the disease in stage three itself, so that it does not progress to stage 4, wherein the macula may be threatened.
Stage 4 ROP develops when neovascularisation progresses to such an extent that it grows into the vitreous gel and leads to traction over the Ridge, and eventually tractional retinal detachment. It is very important that ROP is screened and treated in time so that it does not reach this stage.
Management of stage 4 ROP becomes difficult as it progresses. This is because this is unlike the retinal detachment in adults which has retinal holes and can be settled easily by vitreoretinal surgery. This is the tractional retinal detachment, and the tractional elements have to relieved.
Often vitreoretinal surgery is required by expert eye surgeons, which basically involves vitrectomy and relief of traction over the Ridge, such that the retina can fall back or the traction and retinal detachment progression is prevented. The visual prognosis is always guarded in these cases.
Stage 5 ROP
Stage 5 retinopathy of prematurity (ROP) signifies that total retinal detachment has occured. This is the last stage of retinopathy of prematurity, and the most severe stage too. Since the total retina has detached, it becomes necessary for an eye surgeon to perform eye surgery on these eyes in an attempt to reattach retina.
However, since lot of neovascularisation has occurred, and there exists lot of fibrovascular proliferation which has led to the development of the tractional retinal detachment, this surgery is not easy. This makes the visual prognosis very poor. It requires advanced vitreoretinal surgery to repair retinal detachment, and there are very few eye surgeons in top eye care hospitals across the world where the surgery can be performed.
It needs to be analysed why the child reaches stage five ROP. Possibly it was due to late referral and screening, as many ophthalmologists and paediatricians are still unaware about the disease in developing countries.
Type 1 ROP
Type I Retinopathy of Prematurity signifies the current guidelines to treat ROP promptly within 48 hours.
- Zone I, any stage with plus
- Zone I, stage 3 without plus
- Zone II, stage 2-3 with plus
Type 2 ROP
Type 2 Retinopathy of Prematurity signifies the ROP disease is not severe enough to require treatment. ETROP study classified ROP into type I and type II ROP. If your eye surgeon / ROP specialist labels the child’s eye disease as type II, it means that the child can be followed up in the routine ROP screening program till either the disease regresses or progresses to type 1 ROP to need treatment.
In technical terms, this is how the type to ROP is classified as
- Zone I, stage 1-2 without plus
- Zone II, stage 3 without plus
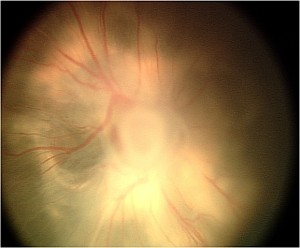
ROP Plus Disease
Plus disease is characterized by abnormal dilation and tortuosity of the retinal arteries and veins at the posterior part of the retina of the eye. This signifies that the disease is active and might progress. Plus disease also causes iris rigidity causing the difficult pupil dilation. Decrease in plus disease is a good sign and might herald disease regression.

AGGRESSIVE POSTERIOR ROP (APROP)
Aggressive Posterior ROP or APROP is a severe form of retinopathy of prematurity which is characterized by fast progression to advances stages. The disease may bypass the early stages 1-3 and progress to stage 5 quickly. The junction is very deceptive and confuses unexperienced doctors easily. Plus disease is characteristically out of proportion to the lack of severity of disease. It needs prompt treatment.
PRETHRESHOLD ROP
Threshold Disease signifies stage of retinopathy of prematurity with ROP in Zone II stage 3 (less than 5 contiguous or 8 non contiguous clock hours) or Zone II stage 3 (5 contiguous or 8 non contiguous clock hours) without plus disease or Zone I, stage 3 with / without plus disease. Many doctors use this as the current criteria of initiating treatment.
THRESHOLD ROP
Threshold Disease signifies stage of retinopathy of prematurity with ROP inZone II, Stage 3 ROP with Plus disease (>5 contiguous or 8 interrupted clock hours) OR Zone I, any stage with plus or stage 3 with no plus. It was earlier criteria of treatment, but is no longer followed now.
* The above resources come from the Internet.